- 首页 > 正文
首个口服周疗方案!Colson博士分享Islatravir联合Lenacapavir的2期研究结果
感染医线 发表时间:2024/3/9 17:35:06
编者按:Islatravir是一款在研的核苷逆转录酶易位抑制剂(NRTTI),而Lenacapavir属于新型的衣壳抑制剂,二者半衰期均较长,作为长效方案的研发热点。Islatravir此前因CD4细胞和淋巴细胞下降不良事件而一度中断临床开发,经降低剂量后与Lenacapavir联合应用的2期试验,在近日举行的CROI大会上首次披露获得积极结果,有望为HIV感染者提供首个全口服的周疗方案。《感染医线》在现场采访了该研究PI、美国社区资源倡议(Community Resource Initiative)研究主任Amy Colson博士。
研究简介
每周一次Islatravir联合Lenacapavir用于HIV感染者的24周疗效和安全性:一项II期研究
背景:核苷逆转录酶易位抑制剂Islatravir(ISL)和衣壳抑制剂Lenacapavir(LEN)具有有效的抗HIV-1活性和药代动力学特征,允许每周一次(QW)口服给药。我们研究了ISL+LEN在HIV-1病毒抑制人群中的疗效和安全性。
方法:在这项2期、随机、开放标签、活性对照研究(NCT05052996)中,接受比替拉韦/恩曲他滨/富马酸替诺福韦艾拉酚胺(B/F/TAF)治疗的病毒学抑制成人被随机分为两组,一组口服ISL 2 mg+LEN 300 mg QW,另一组继续每日服用B/F/TAF。主要疗效终点是第24周时HIV-1 RNA≥50拷贝/mL的参与者比例(FDA Snapshot)。还评估了安全性参数,包括CD4+ T细胞和淋巴细胞绝对计数(ALC)以及不良事件(AE)。
结果:共有104名参与者被随机分组,给药(52人/组)的中位年龄(范围)为40(26-76)岁,其中19人(18.3%)出生时为女性。ISL+LEN组中的1名(1.9%)参与者(其基线HIV RNA为251拷贝/mL)在24周时HIV-1 RNA>50拷贝/mL,随同通过ISL+LEN获得病毒学抑制(24周时病载为64拷贝/mL,39周时<50拷贝/ml)。在第24周时,ISL+LEN组和B/F/TAF组分别有49名(94.2%)和48名(92.3%)参与者维持病毒抑制,其中2名(3.8%)和4名(7.7%)参与者在第24周因中断或错过访视而没有数据。在第24周,CD4+ T细胞计数或ALC的变化未见组间差异(见下表)。39例(75.0%)ISL+LEN受试者和38例(73.1%)B/F/TAF受试者出现不良事件。ISL+LEN参与者中最常见的不良事件包括腹泻(n=7,13.5%)、上呼吸道感染(n=6,11.5%)、关节痛、四肢疼痛和疲劳(各n=3,5.8%)。未报告与研究药物相关的3级或4级不良事件。两名参与者因与药物无关的不良事件(大肠穿孔/肾绞痛/乙型肝炎)而停止了ISL+LEN。
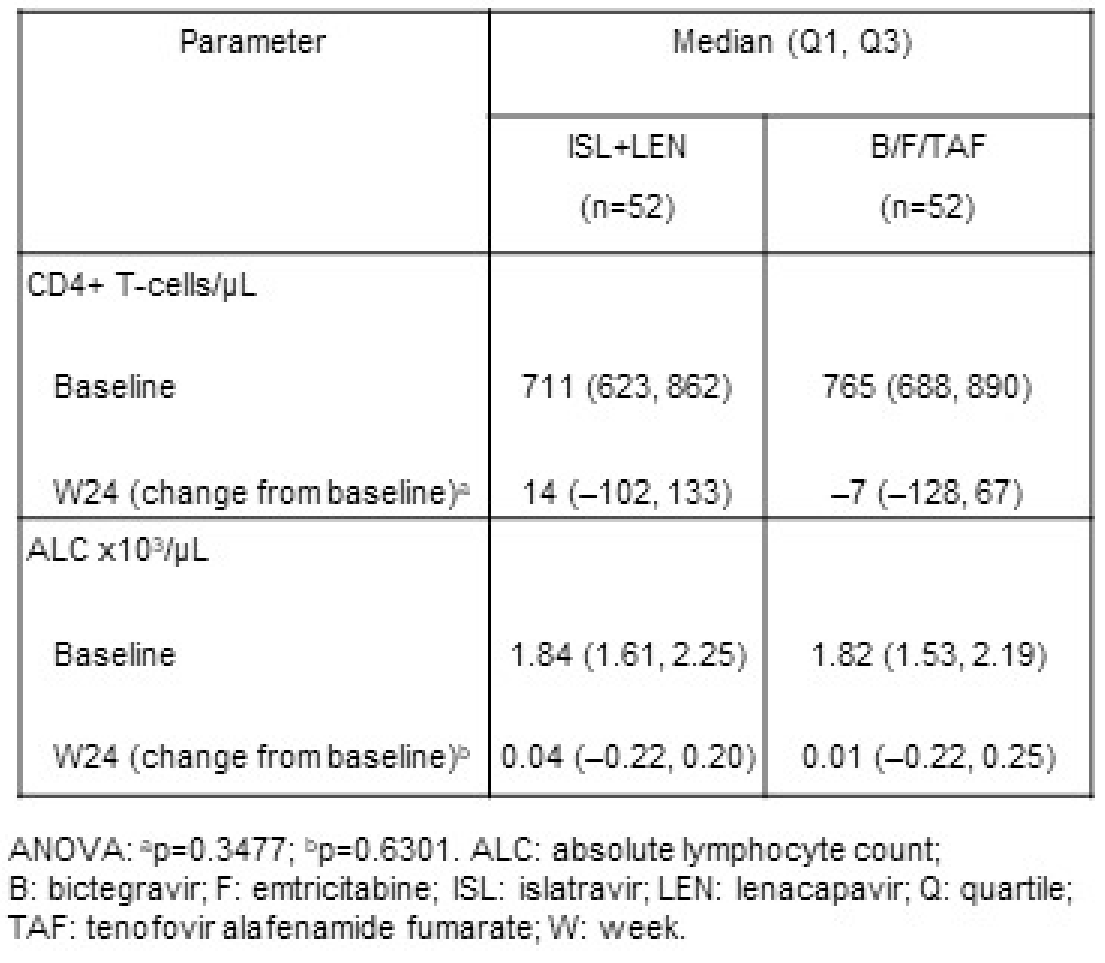
结论:在该2期研究中,ISL+LEN作为第一个口服周疗ARV方案,获得了良好的24周病毒学抑制率,并且耐受性良好。2 mg剂量的ISL没有显示出CD4+ T细胞计数或ALC的临床显著减少,后者在以往较高的每日、每周和每月ISL剂量使用时观察到。
研究者说
01
《感染医线》:能否介绍一下您所汇报的这项研究的主要结果?
Infectious Disease Frontier: What research findings were presented at the conference?
Amy Colson博士:我们今天讨论的研究是一项II期试验,该试验探讨了每周一次的口服Lenacapavir联合Islatravi与标准每日口服方案与克替拉韦/恩曲他滨/丙酚替诺福韦(B/F/TAF))相比的有效性和安全性。入组患者是接受B/F/TAF治疗维持病毒抑制至少24周且CD4细胞计数高于350个/uL,以开放标签的方式随机分配,要么继续他们目前的方案,要么改用新的每周一次的Lenacapavir联合Islatravi。我们在24周时的研究结果显示,两组的病毒学抑制率为92%以上。只有一名服用Islatravir的参与者出现了可检测到的病毒载量,这归因于独特的情况,但随着时间的推移,病毒载量出现了有希望的下降。
Dr. Amy Colson: The study we discussed today was a phase two trial that explored the effectiveness of a once-weekly oral combination therapy consisting of Lenacapavir and Islatravir, compared to the standard daily oral regimen of Bictegravir/Emtricitabine/Tenofovir Alafenamide (B/F/TAF). Participants who had maintained viral suppression on B/F/TAF for at least 24 weeks, with a CD4 count above 350, were randomized in an open-label fashion to either continue with their current regimen or switch to the new weekly combination of Islatravir and Lenacapavir. Our findings at the 24-week mark showed that virologic suppression was maintained equally in both groups at a rate of 92%. Only one participant on Islatravir experienced a detectable viral load, attributed to unique circumstances, yet showed a promising decrease in viral load over time.
02
《感染医线》:感谢您的分享。能否进一步介绍一下安全性表现,尤其是Islatravir根据既往研究而进行了剂量调整?
Infectious Disease Frontier: Thank you for sharing. Can you elaborate on the safety performance of Islatravir in this study, especially regarding any dosage adjustments from previous research?
Amy Colson博士:当然。既往研究中,在较高剂量的Islatravir下观察到CD4细胞计数和淋巴细胞下降的相关问题,促使我们选择每周2mg的较低剂量Islatravir用于该试验。使用早期试验的数据,药代动力学/药效学(PK/PD)模型帮助我们了解Islatravir的剂量与CD4计数下降之间的关系。我们的结果表明,在整个研究过程中,Islatravir-Lenacapavir组和B/F/TAF组之间的CD4或淋巴细胞计数没有显著差异,证实在所选剂量下不存在相关毒性。
Dr. Amy Colson: Of course. Concerns related to CD4 count and lymphocyte declines observed at higher doses of Islatravir in previous studies prompted us to select a lower dose of 2 milligrams per week for this trial. Using data from earlier trials, pharmacokinetic/pharmacodynamic (PK/PD) models helped us understand the relationship between Islatravir's dose and CD4 count declines. Our results indicated no significant difference in CD4 or lymphocyte counts between the Islatravir-Lenacapavir group and the B/F/TAF group throughout the study, confirming the absence of associated toxicities at the chosen dosage.
03
《感染医线》:考虑到新的治疗方案,该研究是否包括耐药突变的监测?
Infectious Disease Frontier: Does the study include monitoring for resistance mutations, considering the novel treatment regimen?
Amy Colson博士:由于大多数参与者保持病毒抑制,因此没有必要进行广泛的耐药性检测。然而,对于在接受治疗前检测到病毒血症的单个病例,耐药检测显示没有针对Islatravir或Lenacapavir的突变,这表明该方案产生耐药性的风险较低。
Dr. Amy Colson: As the majority of participants maintained viral suppression, extensive resistance testing was not necessary. However, for the single case with detectable viremia prior to receiving the treatment, resistance testing showed no mutations against either Islatravir or Lenacapavir, indicating a low risk of developing resistance with this regimen.
04
《感染医线》:您认为周疗口服方案,与一年两次、两个月一次的长效注射剂方案,有怎样的优势或劣势?
Infectious Disease Frontier: How do you compare the advantages or disadvantages of this weekly oral regimen with existing long-acting injectable treatments?
Amy Colson博士:这两种选择都有其独特的好处,适合患者的喜好和生活方式。一些患者喜欢少去诊所注射的便利,而另一些人则更喜欢每周口服的选择,这样可以谨慎行事,避免每天提醒他们的病情。其主要优势是为患者提供选择,使个性化的治疗方法能够适应不同的需求和偏好。
Dr. Amy Colson: Both options have their unique benefits tailored to patient preferences and lifestyles. Some patients appreciate the convenience of less frequent clinic visits for injections, while others prefer a weekly oral option that offers discretion and avoids the daily reminder of their condition. The key advantage is providing choices to patients, enabling a personalized approach to treatment that accommodates different needs and preferences.

Amy Colson, MD, MPH
Community Resource Initiative, Boston, MA, USA
社区资源倡议(Community Resource Initiative)是一家位于美国马塞诸萨州的非盈利性公共卫生机构,旨在整合药物援助、保险导航、预防和研究,提供以客户为中心的整体方法,促进医疗保健领域的社会正义和公平;目标是减少马萨诸塞州的传染病,包括艾滋病毒和结核病;其中的艾滋病毒药物援助计划(HDAP)是马萨诸塞州公共卫生部传染病和实验室科学局艾滋病毒/艾滋病办公室的一项计划。Amy Colson担任该院的研究主任(Director of Research)
来源:《感染医线》
声 明
凡署名原创的文章版权属《感染医线》所有,欢迎分享、转载(开白可后台留言)。本文仅供医疗卫生专业人士了解最新医药资讯参考使用,不代表本平台观点。该等信息不能以任何方式取代专业的医疗指导,也不应被视为诊疗建议,如果该信息被用于资讯以外的目的,本站及作者不承担相关责任。
责任编辑:彭伟彬
相关搜索: HIV